48uep6bbphidvals|155
48uep6bbphidcol4|ID
48uep6bbph|2000F98CTab_Articles|Fulltext
Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder with a wide variety of presentations that may include abdominal pain, bloating, diarrhoea, constipation, or alternating bowel habits.(1) Approximately 20% of the general population has irritable bowel syndrome.(2) It is considered the most common of all gastrointestinal disorders with the prevalence of 5-25 %(3,4). Functional bowel complaints (including IBS) are responsible for 50% of visits to the gastroenterologist.(3) Despite this high prevalence, the cause of IBS is unknown. The diagnostic criteria of IBS include symptoms of bloating, abdominal pain and altered bowel habits.(4) A diagnosis of IBS is made in the absence of alarm symptoms such as fever, anorexia and weight loss.(5,6) Symptoms like bloating, abdominal pain and increased stool frequency are similar to those experienced by subjects with small intestinal bacterial overgrowth (SIBO).5 Using breath-testing techniques, studies from other countries have demonstrated an association between SIBO and IBS. A non-invasive method of diagnosing jejunal bacterial overgrowth is the glucose hydrogen breath test (H2BT) where overgrowth is considered if a rise > 12 ppm in breath hydrogen concentration is observed within 120 minutes of oral administration of glucose.(7) Data on the incidence of small intestinal bacterial overgrowth in patients with IBS from India has not yet been reported. Therefore, the present study was planned.
MATERIALS AND METHODS
225 consecutive patients between the ages of 20 and 65 years attending the Gastroenterology Clinics at PGI, Chandigarh were included in this study. The diagnosis of IBS was entertained if the subjects fulfilled Rome II criteria. One hundred age and sex matched healthy controls were also enrolled in this study.
The exclusion criteria included:
i) History of prior gastric surgery/ vagotomy
ii) History of peptic ulcer and therapy with H2 antagonists/ proton pump inhibitors during the preceding 8 weeks
iii) History of corrosive injury, systemic sclerosis, diabetes, liver cirrhosis and other forms of autonomic neuropathy, hypothyroidism or intestinal pseudo-obstruction
iv) History of treatment with broad-spectrum antibiotics during the one month preceding the test
v) Treatment history with drugs known to interfere with gastrointestinal motility (such as anticholinergics,
antidepressants)
vi) Colonoscopy within a week before H2BT
A detailed history was taken and physical examination was done in all patients. The details of the study were explained and informed consent obtained from each patient.
Investigation of bacterial overgrowth using glucose H2BT:
After taking the basal end expiratory breath reading, all patients were made to drink 50 g glucose in 200 ml water. After drinking 50 g glucose breath samples were collected at 15 minute intervals for a total of two hours. Breath hydrogen concentration was measured by gas chromatography using Model-12 Microlyser (Quintron, USA). An increase in breath H2 concentration >12ppm over baseline value was defined as small intestinal bacterial overgrowth.(8)
Statistical analysis
All results were expressed as mean ± standard deviation (SD). Chi-square test was used to compare the prevalence of small intestinal bacterial overgrowth in IBS patients and healthy controls. A p value less than 0.05 was taken as significant.
Results
Out of 225 patients of IBS, 160 (71.1%) were male while 65 (28.9%) were female. Mean ± SD of age for male patients was 43.5±15.6 years (range 20-65 years) and for female patients was 48.7±16.8 years (range 16-60 years). Of the 100 controls, 65 (65%) were male and 35 (35%) were female. Mean ± SD of age for men in the control group was 45.7±14.5 years (range 15-57 years) and for women was 42. 6±16.52 years (range 18-64 years).
The prevalence of small intestinal bacterial overgrowth was significantly higher in patients with IBS [25 of 225 (11.1%)] as compared to apparently healthy controls [ 1 of 100 (1%)] (Table 1). The prevalence of small intestinal bacterial overgrowth in male and female patients was not statistically significant (Table 2). The pattern of hydrogen concentration in IBS patients with and without small intestinal bacterial overgrowth is shown in Figure 1. The rise (mean ± SD) of peak hydrogen concentration in IBS patients with small intestinal bacterial overgrowth was 15.4 ± 2.8 ppm. While the rise (mean ± SD) of peak hydrogen concentration in IBS patients without small intestinal bacterial overgrowth was 5.4 ± 1.8 ppm.
Table 1. Prevalence of small intestinal bacterial overgrowth (SIBO) in irritable
bowel syndrome patients and controls
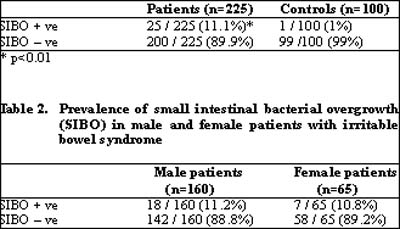
No difference in SIBO +ve prevalence in male and female IBS patients
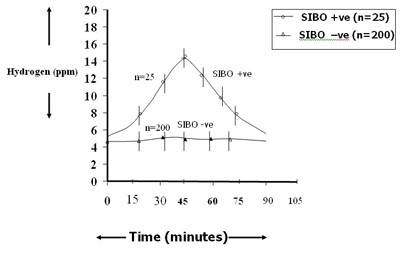
Fig. 1: Pattern of glucose hydrogen breath test in irritable bowel syndrome
patients with and without small intestinal bacterial overgrowth (SIBO)
Discussion
Small intestinal bacterial overgrowth is caused by change in either intestinal motility or defense mechanism of the small bowel and results in reduced clearance of bacteria. The gold standard for the diagnosis of small intestinal bacterial overgrowth involves demonstrating the presence of >105 colony forming units/ml of jejunal fluid. However, this method is impractical, carries the risk of contamination (9) and the results of culture are not always representative. It is commonly believed that culture may give false negative results, especially where obligate anaerobes are concerned.(10) Because of this disadvantage, various breath tests have been developed. Non-invasive breath testing, measuring the production of H2 or methane or both after ingestion of non-fermentable carbohydrate such as glucose8 or lactulose(11) is commonly used to diagnose small intestinal bacterial overgrowth.
Glucose is readily absorbed in the proximal small bowel (jejunum) and in the absence of severe transit abnormalities rarely reaches the colon(12) making it an attractive substrate to detect small intestinal bacterial overgrowth The glucose hydrogen breath test is considered positive if there is a clearly recognisable hydrogen peak, exceeding 10 ppm.(8,13) Therefore, glucose hydrogen breath test has been used in the present study to detect small intestinal bacterial overgrowth.
In this study, we observed a high prevalence (11.1%) of small intestinal bacterial overgrowth in IBS patients when compared with controls (1%). In contrast to our findings, Pimentel et al in 200314 reported a very high prevalence of small intestinal bacterial overgrowth (78%) in IBS patients. They used lactulose as a substrate in their study. The positive breath test obtained using lactulose may have been due to the hydrogen production by colonic bacteria. Galatola et al,(7 )found that up to 29% of patients with irritable bowel syndrome without diarrhoea (faecal weight < 600 g/72 h) and 56% of those with diarrhoea of obscure origin had a positive C14-xylose test, suggesting small intestinal bacterial overgrowth. They concluded that although the C14-xylose test had a high diagnostic value in the setting of clinical research, it could not be used as a routine investigation tool.C14-xylose breath test has been proposed as a very sensitive and specific test for the diagnosis of bacterial overgrowth. However, till date, there is no general agreement on which is the preferred test for the diagnosis of small-intestinal bacterial overgrowth. In a recent study, Posserud et al assessed the prevalence of SIBO, by culture of small-bowel aspirate in 162 patients with IBS.15 SIBO was found in 4% of both patients and controls and the authors concluded that the data did not support an important role for SIBO according to commonly used clinical definitions, in IBS. However as the hypothesis suggesting SIBO as a component of IBS remains attractive, it has led to renewed scrutiny of tests employed to diagnose SIBO and its prevalence in the heterogenous population of irritable bowel syndrome.
To summarise, we have shown that there is a higher prevalence of small intestinal bacterial overgrowth in patients with irritable bowel syndrome from North India as compared to healthy controls.
Reference
1. Talley NJ, Spiller R. Irritable bowel syndrome: a little understood organic bowel disease? Lancet. 2002;360:555–64.
2. Schuster MM. Defining and diagnosing irritable bowel syndrome. Am J Manag Care. 2001;7:S246–51.
3. Talley NJ, Zinsmeister AR, Van Dyke C, Melton LJ 3rd. Epidemiology of colonic symptoms and the irritable bowel syndrome. Gastroenterology. 1991;101:927–34.
4. Wei X, Chen M, Wang J. The epidemiology of irritable bowel syndrome and functional constipation of Guangzhou residents. Zhonghua Nei Ke Za Zhi. 2001;40:517–20.
5. Thompson WG. Irritable bowel syndrome: pathogenesis and management. Lancet. 1993;341:1569–72.
6. Olden KW. Diagnosis of irritable bowel syndrome. Gastroenterology. 2002;122:1701–14.
7. Galatola G, Grosso M, Barlotta A, Ferraris R, Rovera L, Ariano M, Cottino F, De La Pierre M. [Diagnosis of bacterial contamination of the small intestine using the 1 g [14C] xylose breath test in various gastrointestinal diseases] Minerva Gastroenterol Dietol. 1991;37:169–75.
8. Kerlin P, Wong L. Breath hydrogen testing in bacterial overgrowth of the small intestine. Gastroenterology. 1988;95:982–8.
9. Bouhnik Y, Alain S, Attar A, Flourié B, Raskine L, Sanson-Le Pors MJ, et al. Bacterial populations contaminating the upper gut in patients with small intestinal bacterial overgrowth syndrome. Am J Gastroenterol. 1999;94:1327–31.
10. Tabaqchali S. The pathophysiological role of small intestinal bacterial flora Scand J Gastroenterol Suppl. 1970;6:139–63.
11. Rhodes JM, Middleton P, Jewell DP. The lactulose hydrogen breath test as a diagnostic test for small-bowel bacterial overgrowth. Scand J Gastroenterol. 1979;14:333–36.
12. Sellin JH, Hart R. Glucose malabsorption associated with rapid intestinal transit. Am J Gastroenterol. 1992;87:584–9.
13. King CE, Toskes PP. Comparison of the 1-gram [14C]xylose, 10-gram lactulose-H2, and 80-gram glucose-H2 breath tests in patients with small intestine bacterial overgrowth. Gastroenterology. 1986;91:1447–451.
14. Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome. a double-blind, randomized, placebo-controlled study. Am J Gastroenterol. 2003;98:412–9.
15. Posserud I, Stotzer PO, Björnsson ES, Abrahamsson H, Simrén M. Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gut. 2007;56:802–8.