48uep6bbphidvals|577
48uep6bbph|2000F98CTab_Articles|Fulltext
Introduction
Long-term survivors of patients with aplastic anemia may be at high risk for malignant disease. The most common amongst these are myelodysplastic syndromes and acute leukemia. They tend to occur following immunosuppressive therapy or bone marrow transplantation in patients with aplastic anemia. There are few published reports of metachronous solid organ malignancy in survivors of aplastic anemia who have received immunosuppressive therapy or bone marrow transplantation. The most common therapy-related solid organ malignancies that occur in aplastic anemia are head and neck cancers, hepatocellular carcinoma, breast cancer and colorectal cancer. Synchronous solid organ malignancy with aplastic anemia has not been reported in the literature. We report a case of colorectal adenocarcinoma with synchronous aplastic anemia and review the literature concerning the association of aplastic anemia with colorectal cancer.
Case Report
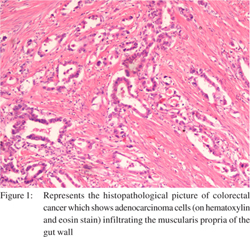
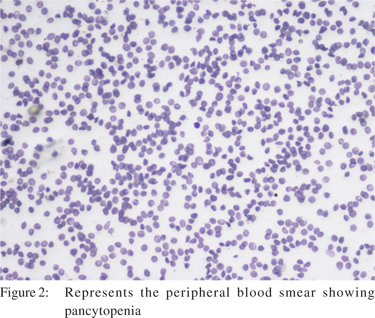
A 32-year-old man, presented with a 2-month history of bleeding per rectum. The patient gave no significant medical history, history of drug intake or any previous hospitalization. There was no family history of hematological illness or malignancy. Rectal examination revealed a circumferential ulcerative growth in the distal rectum, 3 cm from the anal verge up to 7 cm. Punch biopsy of the ulcerative growth revealed well-differentiated adenocarcinoma (Figure 1). On laboratory evaluation his hemoglobin was 5.5 g%, total leucocyte count was 2400/mm3, and platelet count was 30,000/mm3. Peripheral smear described pancytopenia (Figure 2). Bone marrow biopsy suggested aplastic anemia (Figure 3). Computerized tomography showed a mass in the anorectal junction with no perirectal spread or nodes. There was no liver metastasis or ascites. He received preoperative short course radiotherapy of 25 Grays in 5 fractions followed by abdominoperineal resection. The patient’s hemogram and platelet count normalized on transfusion of packed red cell and single donor platelet transfusion. The post-operative period was uneventful and the patient was discharged from the hospital 7 days later.

Discussion
Correlation of solid organ malignancy and hematological disease has rarely been reported in the literature. In the 2 published studies, on gastrointestinal malignancy, in patients with aplastic anemia, only sixteen patients have been reported.[
1-
3] In a review by Socie et al, 860 and 748 patients of aplastic anemia received immuosuppressive therapy and bone marrow transplantation respectively, 7 patients in each group had solid organ malignancy.1 In this review six developed head and neck epidermoid carcinoma,
2 stomach adenocarcinoma,
4 hepatocellular carcinoma and 2 breast carcinoma. None of them had colorectal malignancy. The 10 year cumulative risks of developing solid organ cancers were 18.8% and 3.1% in patients who received immunosuppressive therapy and bone marrow transplantation respectively.[
1]
A recent retrospective review by Kishida et al showed 14 colorectal cancer patients out of 734 patients with hematological disease.[
2] In his review, the highest incidence of colorectal cancer was observed in patients with pure red cell aplasia (18.8%), followed by multiple myeloma (8%) and aplastic anemia (6.5%). Three of 46 patients (6.5%) with aplastic anemia had colorectal adenocarcinoma diagnosed on colonoscopy. All the three patients with colorectal malignancy died of aplastic anemia.[
2]
Synchronous colorectal cancer in patients of aplastic anemia has not been reported in the literature. In this case the patient had an incidental aplastic anemia that was discovered during the work up for colorectal cancer. The pathophysiology behind the development of adenocarcinoma in patients with aplastic anemia has not been well studied.[
4] Large-scale studies and reporting are needed to study the relationship between aplastic anemia and colorectal cancer.
In summary, survivors of aplastic anemia are at risk for development of solid organ malignancy following immunosuppressive therapy or bone marrow transplantation. Patients with aplastic anemia may present with synchronous colorectal adenocarcinoma even before receiving immnosuppressive treatment.
References
1. Socié G, Henry-Amar M, Bacigalupo A, Hows J, Tichelli A, Ljungman P, et al. Malignant tumors occurring after treatment of aplastic anemia. N Engl J Med. 1993;329:1152–7.
2. Socié G, Henry-Amar M, Cosset JM, Devergie A, Girinsky T, Gluckman E. Increased incidence of solid malignant tumors after bone marrow transplantation for severe aplastic anemia. Blood. 1991;78:277–9.
3. Kishida T, Yonezawa M, Shibata Y, Tanaka S, Shinozawa I, Hoshino T, et al. Risk of colorectal cancer in patients with hematologic disease. J Gastroenterol Hepatol. 2000;15:1272–6.
4. Brodsky RA, Jones RJ. Aplastic anaemia. Lancet. 2005;365:1647–56.