|
Sunila Jain1, Vrushali Mahajan1, Mandhir Kumar2
Department of Pathology1
and Gastroenterology2
Sir Ganga Ram Hospital,
Rajinder Nagar, New Delhi, India
Corresponding Author:
Dr. Sunila Jain,
Email: s_isha19@rediffmail.com
48uep6bbphidvals|1350 48uep6bbphidcol2|ID 48uep6bbph|2000F98CTab_Articles|Fulltext Xanthelasmas (xanthomas) are non-neoplastic lesions composed of fat-laden histiocytes commonly seen in the dermis or subcutis. Their occurrence in the stomach is uncommon and can rarely present as gastric polyps mimicking other benign and malignant pathologies[1].Herein, we report an unusual case of xanthelasma of stomach presenting as gastric polyp and illustrate the clinical, endoscopic and histopathological findings. Moreover, we review the literature in order to clarify the clinical and pathological features of this rare pseudoneoplasm.
Case report
A 57-year-old female presented in the gastroenterology outdoor clinic with chief complaints of abdominal pain, dyspepsia and occasional episodes of nausea and vomiting of six months duration. There was no past history of weight loss, diabetes mellitus or any previous surgery. Her general physical
examination was unremarkable. No xanthelasma nodules on skin, eyelids or tendons were seen. Routine hematological investigations and biochemical findings including fasting blood glucose, lipid profile and thyroid function tests were within normal limits. Upper gastrointestinal endoscopy done revealed a small 10 mm x 10 mm polypoidal lesion in the stomach cardia which was removed endoscopically using biopsy forceps. (Figure 1).The rest of the stomach, esophagus and duodenum were unremarkable.
Results
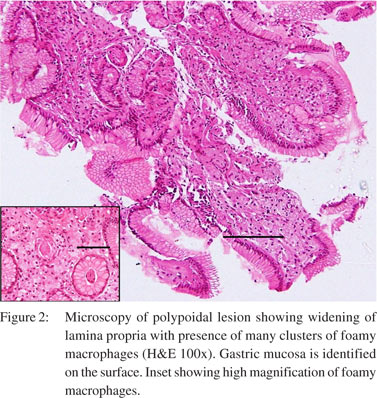
Histopathological examination of the lesion revealed dense aggregates of foamy histiocytes widening the lamina propria (Figure2). On immuno-histochemistry (IHC), these cells were positive for CD68 (Figure 3) and negative for S-100 and cytokeratin. On special stains they were negative for PAS (periodic acid Schiff). No H. pylori or acid fast bacilli were identified and no intestinal metaplasia was seen. The features were compatible with diagnosis of xanthelasma. No etiological agent could be identified. Post polypectomy, there was no recurrence or detection of carcinoma in stomach at the end of the 6-month follow up period.

Discussion
Xanthelasmas or lipid islands are aggregates of large foamy macrophages commonly seen in the dermis, subcutis and sometimes in tendons and synovium. They are known to be commonly associated with hyperlipidemia, diabetes, hypothyroidism, and obstructive liver disease. Xanthelasmas of the gastrointestinal tract are however infrequent and are mostly reported in stomach, while, duodenum and colon are rare sites of involvement [1].In the stomach their incidence is less than 1% and is found more commonly in the antrum especially in the prepyloric area[1,2].They are more frequent in women and its incidence increases with age[2]. The lesions are usually detected incidentally or on autopsy studies for unrelated causes. Clinically, they usually present with vague symptoms of dyspepsia, abdominal pain, nausea and vomiting but these symptoms are not causally related to xanthoma[3].Endosopically, they appear as single or rarely multiple, 0.5 mm to 10mm, yellowish white mucosal patches or plaques[2]. The present case was solitary and located in the cardia. The endoscopic appearances of gastric xanthelasmas may mimic gastric carcinoid tumors or hyperplastic polyp [2].Its etiopathogenesis is still not clear but it is postulated to be an inflammatory response to a focal mucosal damage [4].It is contemplated that healing of gastric injury and chronic inflammation leaves behind lipid-laden debris, which is phagocytised by histiocytes resulting in foam cells [3].These lesions are associated with chronic gastritis, H. pylori infection, intestinal metaplasia and with previous surgery particularly gastrointestinal anastomoses. All of them are predisposing factors for gastric cancers which mandate endoscopic biopsy and careful follow up[2]. Unlike cutaneous xanthomas gastric ones are not found to be directly related to deranged lipid profile [1,2]. The histological appearance of xanthomas is characterized by the presence of aggregates of histiocytes which appear as uniform polygonal cells with abundant foamy cytoplasm filling the lamina propria, usually superficially. As they enlarge, they extend deeper into the submucosa. These macrophages are filled with cholesterol or neutral lipids. Histologically, the differential diagnosis includes granular cell tumor, signet ring cell carcinoma, Malacoplakia, Whipple’s disease, glycogen storage disorders and mycobacterium avium intracellulare infection (MAIC) [5] (Table1). Xanthomas are considered benign lesionsthat require polypectomy. The clinical significance of gastric xanthelasmas is not completely elucidated. A correlation with gastric cancer has been implicated by some authors [6].A careful examination of the remaining gastric mucosa and follow-up has been suggested. In the present case no correlation with carcinoma could be established. In view of the rarity of this coexistence, it can be argued that this coexistence maybe a incidental rather than a precursor pathology.


References
- Andrejiæ BM, Bo•aniæ SV, Solajiæ NS, Djolai MA, Levakov AM. Xanthomas of the stomach: a report of two cases. Bosn J Basic Med Sci. 2012;12:127–9.
- Gursoy S, Yurci A, Torun E, Soyuer I, Guven K, Ozbakir O, et al. An uncommon lesion: Gastric Xanthelasma. Turk J Gastroenterol.2005;16:167–70.
- Hilabi I, Yassen M, Vesoulis Z. Multiple gastric xanthomas in a 3 year old patient. Gastroenterol Hepatol (N Y). 2010;6:181–3.
- Bassullu N, Turkmen I, Uraz S, Yagiz Korkmaz P, Memisoglu R, Gultekin OS, et al. Xanthomatous hyperplastic polyps of the stomach: clinicopathologic study of 5 patients with polypoid gastric lesions showing combined features of gastric xanthelasma and hyperplastic polyp. Ann Diagn Pathol. 2013;17:72–4.
- Lewin K.J., Appelman H.D. Tumors of esophagus and stomach, Atlas of tumor pathology; 3rd edition, Fascicle 18; Armed forces institute of pathology, Washington DC ;1995. Chapter 14-Mesenchymal tumors and tumor like proliferations. 405–52.
- Sekikawa A, Fukui H, Maruo T, Tsumura T, Kanesaka T, Okabe Y, et al. Gastric xanthelasma may be a warning sign for the presence of early gastric cancer. J Gastroenterol Hepatol. 2014;29:951–6.
|