48uep6bbphidvals|154
48uep6bbphidcol4|ID
48uep6bbph|2000F98CTab_Articles|Fulltext
Acute pancreatitis is a common cause of acute abdomen. The aetiological factors are varied and may include biliary stones, alcoholism, trauma, drugs, and metabolic and idiopathic causes. Most patients have acute oedematous pancreatitis with interstitial inflammation and favourable clinical outcome. Some patients suffer acute necrotising pancreatitis with severe parenchymal necrosis and rapid deterioration to multiple organ failure frequently requiring organ support. Several scoring systems are available involving clinical and laboratory data, which can differentiate mild from severe pancreatitis. The aim of this prospective study is to analyse data concerning aetiology, severity of disease process and outcome in cases of acute pancreatitis.
METHODS
In this prospective study 45 cases of acute pancreatitis were admitted between August 2002 and December 2003.The diagnosis was ascertained by clinical assessment, measurement of hyperamylasaemia and imaging techniques (USG/CT). The severity of the disease process was assessed by the Acute Physiology and Chronic Health Evaluation (APACHE) scoring system. Those with APACHE score >9 were diagnosed as cases of severe acute pancreatitis (SAP). Laboratory investigations at the time of admission included measurement of serum amylase, haematocrit, total and differential leukocyte counts, blood urea and serum electrolytes, serum calcium, random blood glucose, liver enzymes, arterial blood gases and ultrasound. Contrast enhanced computed tomography (CECT) scan was done between the 4th and 8th days of admission and the presence and extent of necrosis was determined. The use of endoscopic retrograde cholangiopancreatography (ERCP) + sphincterotomy was reserved for patients with acute pancreatitis due to biliary calculi with cholangitis. ERCP or magnetic resonance cholangiopancreatography (MRCP) was also used if there was relapse of the disease and when CT scan suggested architectural distortion of the pancreatic parenchyma or duct. The treatment protocol in mild pancreatitis included bowel rest and parenteral analgesics (diclofenac or opioids). No antibiotics were used in mild cases. The treatment protocol in SAP comprised bowel rest, oxygen, nasogastric drainage, parenteral antibiotics (ciprofloxacin or imipenem), parenteral opioids, nutritional support and organ support as indicated. All patients were followed up by close monitoring and serial ultrasound or CT scan. The data regarding aetiology, severity and outcome in acute pancreatitis were analysed.
RESULTS
A total of 45 patients diagnosed with acute pancreatitis were evaluated in this prospective study. Out of 45 patients, 33 were male and 12 were female. The mean age of the patients was thirty years. The causes of pancreatitis (as detailed in Table 1) were as follows: 16 (35.5%) due to alcoholism, 10 (22.2%) due to gallstones, 9 (20%) due to trauma, 6 (13.3%) due to idiopathic causes, and 4 (8.8%) following ERCP. 34 patients had mild pancreatitis and 11 had severe pancreatitis. Of the 34 patients with mild pancreatitis 14 (41.1%) were due to alcoholism, 8 (23.5%) due to gallstones, 6 (17.6%) posttraumatic, 4 (11.7%) idiopathic and 2 (5.8%) post-ERCP. The aetiology of mild pancreatitis is presented in Table 2. The causes of SAP were 3 (27.2%) post-traumatic, 2 (18.1%) idiopathic, 2 (18.1%) due to gallstones, 2 (18.1%) due to alcoholism and 2 (18.1%) post-ERCP (Table 3).
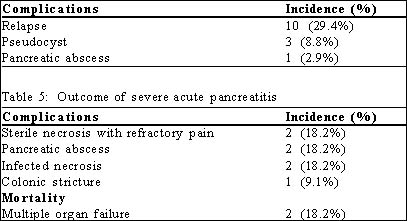
The outcome of mild pancreatitis was evaluated (Table 4). All patients recovered in 5 to 7 days. 3 patients developed pseudocyst. On a 12-week follow up, 2 patients with pseudocyst of 5.5 cm and 7.5 cm, respectively, responded to conservative treatment and 1 patient with pseudocyst of 12.5 cm required surgery in the form of a cystogastrostomy. 1 patient had a pancreatic abscess. This patient was an elderly female with idiopathic pancreatitis who then underwent CT-guided aspiration, leading to resolution. 10 patients had relapse of pain of whom 8 were alcoholics and 2 had idiopathic pancreatitis. ERCP/MRCP when performed in these 10 patients
demonstrated pancreatic parenchymal and ductal distortion in 7 of them. 1 of these 7 patients had pancreatic ductal stricture in the body and underwent lateral pancreaticojejunostomy with satisfactory outcome. The rest were treated with pancreatic enzyme supplements.
Table 1: Aetiology of acute pancreatitis (n=45)
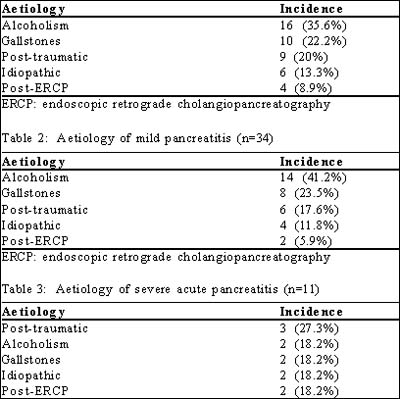
ERCP: endoscopic retrograde cholangiopancreatography
Of the 11 patients with SAP, 2 developed infected pancreatic necrosis, diagnosed on CT-guided aspiration and microbiological study. Both patients were treated successfully by laparotomy with necrosectomy and closed drainage. The resultant external fistula in the 2 cases took 11 and 16 days respectively, to spontaneously resolve. 2 patients developed pancreatic abscess of which 1 was an elderly patient with a 4 cm abscess. She underwent CT-guided aspiration and received antibiotics based on the antibiogram, which led to resolution of the abscess. The other patient was treated with laparotomy and external drainage. 2 patients developed extensive sterile pancreatic necrosis (diagnosed on CECT scan) and recurrent post-prandial pain; 1 of them underwent necrosectomy with closed drainage in the 4th week. The external fistula closed by the 22nd day on conservative management and in this case octreotide was instilled subcutaneously from day 10 through 14 at a dose of 50 mg twice daily. Another patient who developed sterile pancreatic necrosis was managed conservatively on parenteral fluids and nutrition and had a prolonged hospital stay. One young patient successfully treated for SAP following abdominal trauma developed subacute intestinal obstruction after 6 months of discharge and was admitted twice for the same problem. A barium series was done which revealed a colonic stricture at the transverse colon close to the splenic flexure, which was then treated by colonic resection. Amongst the SAP patients, 2 died due to multiple organ failure. The results of outcome for mild and severe acute pancreatitis are shown in Tables 4 and 5.
Table 4: Outcome of mild pancreatitis
DISCUSSION
Acute pancreatitis has variable aetiology. In our study alcohol was the commonest cause (35.5%), although gallstones have been implicated as the commonest cause in other studies. In another series from our country it was seen that 60% of cases with acute pancreatitis were gall stone induce(1)The prognostic criterion used in our study was the APACHE scoring system, which has been reported to identify 63% of SAP cases at 0 hours.(2)
In the mild pancreatitis group we did not use prophylactic antibiotics as prophylaxis for pancreatic sepsis. Only 1 out of 34 patients developed infected pancreatic necrosis with abscess formation which was treated successfully by CT guided aspiration and parenteral antibiotics. Relapse of pain was seen in 10 of 34 patients of mild pancreatitis in a 6-month follow-up. In 7 of these 10 cases, parenchymal calcification or ductal irregularity + calculi /stricture were found on ERCP/MRCP; this may be attributed to the cause or sequelae of acute pancreatitis. Pancreaticojejunostomy in 1 patient with ductal stricture, and pancreatic enzyme supplements in the remaining 9 patients resulted in satisfactory control of pain.
Out of 11 cases of SAP we used ciprofloxacin in 6 cases and imipenem in 5 cases. 1 patient from each group died due to multiple organ failure. 1 patient from each group developed sterile necrosis with symptoms of recurrent postprandial pain but the one treated with ciprofloxacin needed surgery in the form of necrosectomy in the 5th week. The other patient was managed on intravenous alimentation, analgesics and antibiotics necessitating a prolonged hospital stay. (3)patients in the ciprofloxacin group developed infected pancreatic necrosis with abscess but only 1 in the imipenem group did so. Literature also supports the use of imipenem in reducing pancreatic and extrapancreatic sepsis although it neither reduces the need for surgical intervention nor the incidence of organ failure and death.(3)
The role of necrosectomy in sterile pancreatic necrosis is controversial, although the Santorini Consensus Conference(4) has advocated its use in patients with recurrent postprandial pain, persistent systemic inflammatory response syndrome and rapidly deteriorating organ failure. In our series, (2) patients developed extensive sterile necrosis with recurrent severe postprandial pain. The first patient was treated with necrosectomy and the other patient was managed conservatively. However, both hospital stay and residual pain were more in the latter. The timing of necrosectomy in such cases is thought to be considerably important. Evidence suggests that delayed intervention leads to improved results compared to early intervention - a concept that we did follow in this study.(5)
Of the 2 pancreatic abscess cases, (1) patient who was unfit for anaesthesia due to co-morbid cardiac illness underwent CT guided aspiration and appropriate antibiotic treatment based on an antibiogram. This led to resolution of sepsis and abscess and thus suggests its role in select cases. One case of posttraumatic SAP in a young boy presented (4) months later with recurrent subacute intestinal obstruction. A barium study of the gut demonstrated a colonic stricture at the transverse colon near the splenic flexure and the patient underwent colonic resection. This is a rare complication of acute pancreatitis.(6)
CONCLUSION
To summarise, we found that alcohol was the commonest cause of acute pancreatitis in our setting. The aetiology of severe acute pancreatitis is however, varied. The treatment of mild pancreatitis is usually rewarding with good outcome even without the use of antibiotics. The outcome of severe acute pancreatitis can be improved by appropriate timing of necrosectomy, CT-guided aspiration of pancreatic abscess in select cases together with careful assessment and monitoring.
REFERENCES
1. Kumar S, Pandey HI, Jangbahadur AS et al. Prognostic factors in acute necrotizing pancreatitis. GI Surgery Annual. 2003;10:119–28.
2. Larvin M, McMohan MJ. APACHE-II Score for assessment and monitoring of acute pancreatitis. Lancet. 1989;2:201–5.
3. Pederzoli P, Bassi C, Vesentini S, Campedelli A. A randomized multicenter clinical trial of antibiotic prophylaxis of septic complications in acute necrotizing pancreatitis with imipenem. Surg Gynecol Obstet. 1993;176:480–3.
4. Dervenis C, Johnson CD, Bassi C, Bradley E, Imrie CW, McMahon MJ, et al. Diagnosis, objective assessment of severity and management of acute pancreatitis. Santorini consensus conference. Int J Pancreatol. 1999;25:195–210.
5. Mier J, Leon EL, Castillo A, Robledo F, Blanco R. Early versus late necrosectomy in severe necrotizing pancreatitis. Am J Surg. 1997;173:71–5.
6. Mair WS, McMahon MJ, Goligher JC. Stenosis of the colon in acute pancreatitis. Gut. 1976;17:692–5.