48uep6bbphidcol2|ID
48uep6bbphidvals|1736
48uep6bbph|2000F98CTab_Articles|Fulltext
Alpha-fetoprotein (AFP) is a glycoprotein that is normally produced during gestation by the fetal liver and the yolk sac.
1 Elevation of serum AFP is considered pathological in adults. In clinical practice, the estimation of AFP in serum is used to screen high risk patients of chronic liver diseases for hepatocellular carcinoma. However, AFP levels may be elevated in patients of primary gastric carcinoma
2 as well as other malignancies.
3-9 (
Table 1) AFP producing gastric cancer (AFPGC) constitutes only about 2.7% to 8% of all gastric cancers.
10 They have high metastatic potential and possibility of vascular invasion, liver and lymph nodal metastases resulting in poor prognosis.
2 In situations where associated liver mass is seen, it may be mistaken for coexistent hepatocellular carcinoma, like the index case.
We thus report this rare case of AFPGC, an entity which the treating physicians need to be familiar with.
Case Report
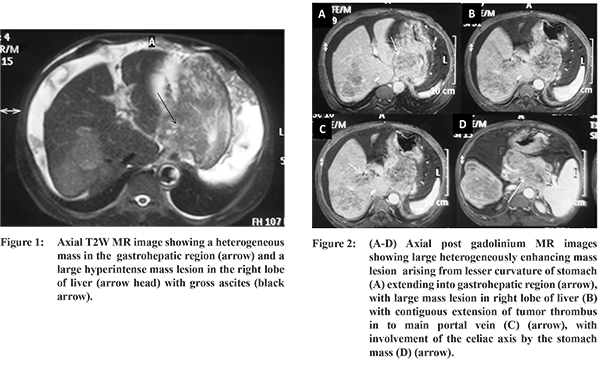
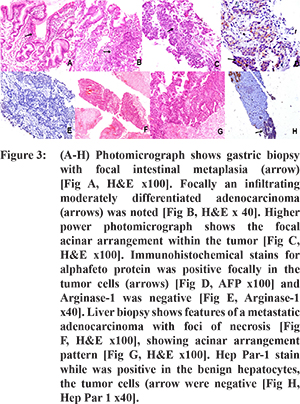
A 47 year-old male presented to the liver clinic of our hospital with dull aching pain in the upper abdomen for one and a half months. He had history of anorexia and weight loss. There was no history suggestive of chronic liver disease such as abdominal distension, jaundice or encephalopathy. There was no history of blood transfusion or prior surgery. On physical examination, he was anicteric and had no lymphadenopathy or pedal edema. Liver was palpable, which was hard in consistency with irregular margin. Routine blood investigations revealed hemoglobin of 9.1 g/dL, total leucocyte count of 11,100 per cu mm and a platelet count of 181,000 per cu mm. The liver and renal function tests were within normal limits. Serum AFP was markedly elevated (58,618 ng/ml). Multiphasic MRI abdomen revealed diffuse gastric wall thickening involving the body and the antral region with multiple lesions in the right lobe of liver that were heterogenously enhancing. Conglomerate of enlarged lymph nodes were present in the lesser and greater omentum, subpyloric region and the splenic hilum with omental and peritoneal metastases. (Figure 1,2) Based on the elevated serum AFP level and MR imaging, a possibility of hepatocellular carcinoma was kept. Further, upper gastrointestinal endoscopy confirmed the findings of MRI and a pyloric antral biopsy was done. This showed moderately differentiated adenocarcinoma, with predominant diffuse sheets of tumor cells resembling fetal hepatocytes and focal acinar arrangements. Subsequently, an ultrasound guided biopsy of the liver mass was performed which revealed features of adenocarcinoma. Immunohistochemical stains performed in the gastric biopsy showed focal positivity for alpha-fetoprotein and CdX2 and the cells were negative for Arginase-1. Liver biopsy showed features of a metastatic adenocarcinoma with acinar arrangement, along with foci of necrosis. The hepatic tumor was negative for HepPar-1 and CK.7 (Figure 3) Diagnosis of AFP producing gastric carcinoma with disseminated metastases was made. The patient was very sick and once the diagnosis and prognosis was revealed, he opted for palliation alone.
Discussion
AFPGC generally occurs in the sixth to seventh decade and pyloric antrum is the most frequent site. AFPGC has multiple phenotypes including gastric hepatoid, intestinal and signet ring type.
11 Liver metastasis (14.3%-75.6%) is one of the main features of hepatoid variant. Gastric hepatoid adenocarcinoma (GHA) has a striking morphologic similarity to hepatocellular carcinoma (HCC).
11 The tumor cells in the hepatoid foci resemble the morphology of HCC, and the immunohistochemistry can be positive for AFP, PIVKA-II, alpha-1 antitrypsin, alpha-1 antichymotrypsin and albumin. AFP production in AFPGC is thought to be due to hepatoid differentiation of tumour cells.
11 SALL4 (Sal-like protein 4) is an oncofetal protein similar to AFP and represents fetal gut differentiation in gastric carcinoma. SALL4 is a sensitive marker for AFP-producing gastric carcinoma and is especially useful to distinguish hepatoid gastric carcinoma from hepatocellular carcinoma.
12 Various reports have shown that AFP producing carcinoma of the stomach has a more aggressive behavior than the common gastric cancers in the form of higher incidence of vascular invasion, lymph node and liver metastasis.
13 Data regarding optimum therapy of AFPGC is sparse. The treatment is similar to that of common gastric adenocarcinoma. Surgical management of an early primary tumor, if feasible, is the indicated approach. Adjuvant chemotherapy and radiotherapy should be given according to current gastric cancer indications, despite the fact that no specific data on adjuvant treatment of AFPGC is available.
References
- Bergstrand CG, Czar B. Demonstration of a new protein fraction in serum from the human fetus. Scand J Clin Lab Invest. 1956;8:174.
- Liu X, Cheng Y, Sheng W, et al. Clinicopathologic features and prognostic factors in alpha-fetoprotein-producing gastric cancers: analysis of 104 cases. J Surg Oncol. 2010;102:249-55.
- Saito S, Hatano T, Hayakawa M et al. Studies on alpha-fetoprotein produced by renal cell carcinoma. Cancer. 1989;63(3):544-9.
- Ng WK, Ng WF et al, Elevated serum alpha-fetoprotein in a patient with undifferentiated carcinoma of the gall bladder. J Clin Pathol. 1995;48(11):1061-3.
- Yoshino I, Hayashi I, Yano T, et al. Alpha-fetoprotein-producing adenocarcinoma of the lung. Lung Cancer. 1996;15:125-130.
- Mueller SB, Micke O, Herbst H, et al. Alpha-fetoprotein-positive carcinoma of the pancreas: A case report. Anticancer Res. 2005;25:1671-1674.
- Blandamura S, Vendraminelli R, Aversa S, Fedrigo M. Collecting duct carcinoma of kidney producing alpha-fetoprotein. Eur J Surg Oncol. 2005;31:1039-1041.
- Crocoli A, Madafferi S, Jenkner A, et al. Elevated serum alpha-fetoprotein in Wilms tumor may follow the same pattern of other fetal neoplasms after treatment: evidence from three cases. Pediatr Surg Int. 2008;24:499-502.
- Lu CH, Chou WC, Hung YS, et al. Alpha-fetoprotein-producing transitional cell carcinoma of the urinary bladder: a case report. Int Urol Nephrol. 2009;41:567-570.
- Shibata Y, Sato K, Kodama M et al. a-fetoprotein-producing early gastric cancer of the remnant stomach: report of a case. Surg Today. 2007, 37:995-999.
- Ishikura H, Fukasawa Y, Ogasawara K et al. An afp-producing gastric carcinoma with features of hepatic differentiation. A case report. Cancer. 1985;56:840-8.
- Ushiku T, Shinozaki A, Shibahara J et al. SALL4 represents fetal gut differentiation of gastric cancer, and is diagnostically useful in distinguishing hepatoid gastric carcinoma from hepatocellular carcinoma. Am J Surg Pathol. 2010;34(4):533-40.
- Xiaowen Liu et al. Clinicopathologic Features and Prognostic Factors in Alpha-Fetoprotein-Producing Gastric Cancers: Analysis of 104 Cases. Journal of Surgical Oncology. 2010;102:249-255.