48uep6bbphidcol2|ID
48uep6bbphidvals|1783
48uep6bbph|2000F98CTab_Articles|Fulltext
Common variable immunodeficiency (CVID) is a heterogeneous disorder of B-cells, which is characterized by marked reduction of serum levels of IgG, IgA or IgM, recurrent bacterial infections, impaired antibody response of B cells, and normal or near-normal T-cell immunity.
1 We describe the first case from an Indian subcontinent of a patient with CVID who developed adenocarcinoma of the stomach at an early age.
Case Report
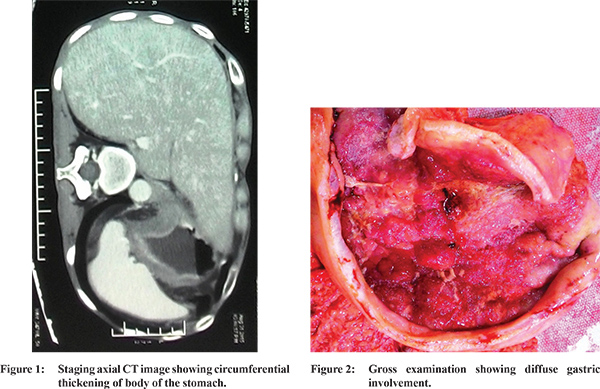
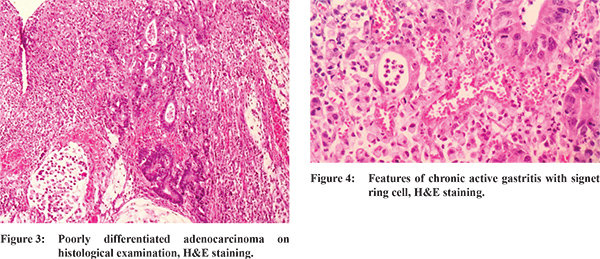
Our patient was a 39 years south Indian male with congenital hypothyroidism, diagnosed with common variable immunodeficiency disease for 20 years. He required a monthly infusion of intravenous immunoglobulin. He was suffering from chronic cough and diarrhea and was diagnosed to have chronic bronchitis with Crohn’s disease and was on azathioprine therapy for the same for last one year. He recently had complaints of loss of weight of 6 kg over a period of two-months with intermittent vomiting. A gastroscopy was done to investigate these complaints. An irregular mass involving the body was seen on endoscopy, and biopsies from the mass were taken. Histology showed poorly-differentiated adenocarcinoma with signet ring cells. Staging computed tomography (CT) (Figure 1) showed circumferential thickening of the body with no serosal involvement or distant spread. The patient underwent a D2 total gastrectomy. Intraoperatively, there was a mass involving body of the stomach (Figure 2) with enlarged perigastric lymph nodes. No liver metastasis or peritoneal disease was present. Following total gastrectomy, a Roux-enY antecolic gastrojejunostomy with a functional side to side jejunojejunostomy was performed using GI staplers. Post operatively, his abdominal drain output was more than one liter for initial 5 days and albumin level was 2 gm/dl. He was given intravenous albumin infusion. He developed breathlessness and was diagnosed to have bilateral basal pneumonitic patch on day 7 and required high end antibiotic, antifungal therapy and ventilator support.In spite of which his clinical condition deteriorated and he succumbed to pneumonia on post operative day 10. Histology confirmed poorly differentiated signet ring cell adenocarcinoma (Figure 3,4). Pathological staging was T3N2M0 with 8 out of 21 nodeswere involved. The resection margin of the specimen was not involved.
Discussion
Common Variable Immunodeficiency (CVID) is associated with a broad spectrum of symptoms related to infections, chronic lung diseases, autoimmune diseases, and tumors. The mean age of diagnosis is 29 years for males and 33 years for females.
1 The 20-year survival rate after diagnosis of this condition is 64% for males and 67% for females.1 Patients with CVID are at an increased risk of malignancy, especially lymphoma and gastric cancers. An increased risk of gastric cancer in patients with CVIDs was recognized in 1985, when a prospective study of 220 patients with CVIDs followed for 11 years reported a 47-fold increased risk although only 7 patients were diagnosed to have gastric malignancy.
2 Outcome study of large CVID cohort followed for a median period of 7 years found that the absolute risk of gastric carcinoma is low.
1 The Oxford database studies showed that from a total of 116 patients with CVIDs only one patient was diagnosed to have gastric adenocarcinoma.
3 The mechanisms underlying an increased frequency of gastric cancer in CVIDs are not understood. It is hypothesized that H. pylori plays a role in the gastric carcinogenesis of patients with CVID.4 In 1999, Zullo et al studied gastric pathology in patients with CVID and reported 14 of 34 patients had H. pylori infection, 80% of which was associated with chronic atrophic gastritis.
4 In this series, two of 34 had neoplasia (one adenocarcinoma and one highgrade dysplasia), consistent with an increased risk of gastric cancer in CVIDs. Autoimmunity is a well-recognized complication of CVIDs. In one study, 69 patients evaluated over a period of 10 years, 22 (31.9%)patients were diagnosed to have 13 autoimmune diseases, most frequent being the hematological disorders and hypothyroidism. Three (4.3%) patients developed B cell lymphoma, four (5.8%) hadstomach adenocarcinoma and one breast cancer.
5 Our case emphasizeson surveillance of CVID patients for gastric cancer, with a shorter follow up duration, which may present at an early age and need for combined multi institutional efforts for formulating guidelines for the same.
References
- Cunningham-Rundles C, Bodian C. Common Variable Immunodeficiency: clinical and immunological features of 248 patients. Clin Immunol. 1999;92:34-48.
- Kinlen LJ, Webster AD, Bird AG et al. Prospective study of cancer in patients with hypogammaglobulinaemia. Lancet. 1985;1:263-6.
- Lucas M, Lee M, Lortan J, Lopez-Granados E, Misbah S, Chapel H. Infection outcomes in patients with common variable immunodeficiency disorders: relationship to immunoglobulin therapy over 22 years. J Allergy Clin Immunol. 2010;125:1354-60.
- Zullo A, Romiti A, Rinaldi V et al. Gastric pathology in patients with common variable immunodeficiency. Gut. 1999;45:77-81.
- Fernández Romero DS1, Juri MC, Paolini MV, Malbrán A. Common variable immunodeficiency. Epidemiology and clinical manifestations in 69 patients. Medicina (B Aires). 2013;73(4):315-23.