48uep6bbphidcol2|ID
48uep6bbphidvals|3034
48uep6bbph|2000F98CTab_Articles|Fulltext
Gastric volvulus as a clinical entity was first described by Berti in 1866 during an autopsy on a female patient.1 Gastric volvulus occurs when the stomach rotates more than 180 degrees either along its longitudinal (organoaxial) or transverse (mesenteroaxial) axis. Acute gastric volvulus, characterised by Borchardt’s triad of acute epigastric pain, retching with inability to vomit, and difficulty to pass a nasogastric tube, can lead to strangulation of the stomach with resultant perforation and septic shock and requires urgent surgical attention.2,3 On the other hand, chronic gastric volvulus presents with vague symptoms such as episodic upper abdominal pain, bloating, hiccups, and/or chronic anemia.
Case Report
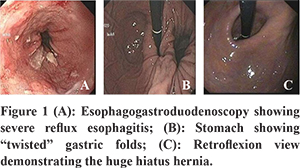
A 67-year-old male patient with no significant past medical history was referred to us as part of evaluation for his anemia. The patient on further probing gave history of recurrent, self-limiting, spasmodic, on-and-off upper abdominal pain which was unrelated to meals and was nonradiating. He had no other associated symptoms during these pain episodes. Physical examination was non-contributory except for mild pallor. Laboratory evaluation showed a haemoglobin and haematocrit of 7.60 and 23 with a platelet count of 4,26,000. His iron studies pointed towards iron-deficiency anemia with a ferritin level low at 6.1 (21.81 to 274.6 ng/mL). Stool for fecal occult blood was positive. He was subjected to esophagogastroduodenoscopy which revealed severe, Los Angeles grade D reflux esophagitis. Upon entering the stomach, the gastric folds appeared “twisted and turned” and there was difficulty negotiating through the antrum and pylorus indicative of an organoaxial gastric volvulus (Figure 1).
The diagnosis was further confirmed with barium study which demonstrated type 4 hiatus hernia with intrathoracic stomach and associated organoaxial gastric volvulus with no evidence of obstruction noted on the study (Figure 2). Since the patient only had on and off pain which did not limit his day-to-day activities, he was offered conservative management and placed on iron and folic acid supplements with regular followup.
Discussion
Gastric volvulus is a rare clinical entity which occurs when the stomach makes an abnormal “twist” around its ligamentous attachments and the presentation depends on the rapidity of onsetand the degree of gastric twist.4 Primary gastric volvulus occurs when the ligaments of the stomach became lax. The more common secondary volvulus occurs due to a paraesophageal hernia. Other causes include congenital or traumatic diaphragmatic hernia, eventration of the diaphragm, wandering spleen, or adhesions.5
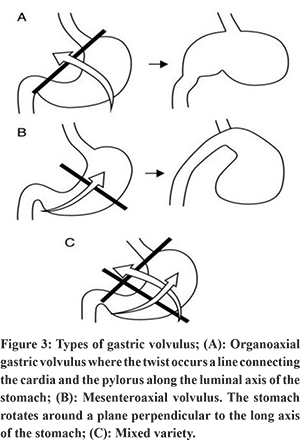
Based on the axis of rotation, gastric volvulus can be of three types (Figure 3). Organo-axial gastric volvulus is the most common variant and occurs when the stomach rotates around its long axis. This variety of volvulus isusually associated with para-esophageal hernias or diaphragmatic eventration. The second type of gastric volvulus is the mesentero-axial volvulus, which is less common and occurs around the short axis of the stomach, which runs from the center of the greater curvature to the porta hepatis. The third and rarest form is a combination of both the organo-axial and mesentero-axial variants.
While acute gastric volvulus is an acute surgical emergency, chronic gastric volvulus can present with subtle symptoms of chronic repeated upper abdominal pain, dysphagia, bloating, anemia, hiccups, etc.6 A definitive diagnosis requires imaging as well OGD. A retrocardiac, air-filled mass may be noted on chest x-ray.7 Barium studies of the upper gastrointestinal tract confirm the diagnosis and are both sensitive and specific.8,9,10,11 CT scan has a high sensitivity and specificity for the diagnosis of gastric volvulus and shows an abnormally located antrum at the same level or higher than the gastric fundus. A “swirl sign” may be evident on CT where in the esophagus and stomach rotate around each other on transverse plane images.4 Management depends on the acuteness of onset, presence of gastric ischemia, and presence of comorbidities. After intravenous fluid resuscitation and nasogastric decompression, volvulus should be reduced endoscopically and/or laparoscopically.
Conclusion
Although chronic gastric volvulus is a rare clinical entity, clinicians should consider it in the differential diagnosis of chronic iron deficiency anemia and chronic episodic upper abdominal pain. EGD and barium studies remain the diagnostic tests of choice in diagnosing gastric volvulus. Given that chronic gastric volvulus is a non-life-threatening condition, symptom-based nonoperative management should be considered in such patients.
References
- Berti A: Singolareattorcigliamentodell’esofago col duodenosequito da rapidamorte. Gazz Med Ital 1866, 9:139-141.
- Rashid F, Thangarajah T, Mulvey D, et al. A review article on gastric volvulus: a challenge to diagnosis and management. Int J Surg 2010;8:18–24.
- Chau B, Dufel S. Gastric volvulus. Emerg Med J 2007;24:446–7.
- Han BK, Levin TL, Murphy R, Blitman NM, Ramos C. Gastric volvulus in children: the twists and turns of an unusual entity. PediatrRadiol. 2008;38(3):297-304.
- Chen DP, Walayat S, Balouch IL, Martin DK, Lynch TJ. Abdominal pain with a twist: a rare presentation of acute gastric volvulus. J Community Hosp Intern Med Perspect. 2017 18;7(5):325-328.
- McElreath DP, Olden KW, Aduli F. Hiccups: a subtle sign in the clinical diagnosis of gastric volvulus and a review of the literature. Dig Dis Sci 2008;53:3033–6.
- Shivanand G, Seema S, Srivastava DN, et al. Gastric volvulus: acute and chronic presentation. Clin Imaging 2003;27:265–8.
- Gourgiotis S, Vougas V, Germanos S, et al. Acute gastric volvulus: diagnosis and management over 10 years. Dig Surg 2006;23:169–72.
- Millet I, Orliac C, Alili C, et al. Computed tomography findings of acute gastric volvulus. Eur Radiol2014;24:3115–22.
- Teague WJ, Ackroyd R, Watson DI, et al. Changing patterns in the management of gastric volvulus over 14 years. Br J Surg 2000;87:358–61.
- Carter R, Brewer LA 3rd, Hinshaw DB. Acute gastric volvulus: a study of 25 cases. Am J Surg 1980;140:99–106.