Kirti Gupta, Anjali Solanki, RK Vasishta
Department of Histopathology,
Post Graduate Institute of Medical Education and Research,
Chandigarh – 160012, India
Corresponding Author:
Dr. Kirti Gupta
Email: kirtigupta10@yahoo.co.in
48uep6bbphidvals|478 48uep6bbph|2000F98CTab_Articles|Fulltext Neurogenous hyperplasia of the appendix or appendiceal neuroma, first described by Pierre Masson in 1928 is a relatively common entity characterized by obliteration of the lumen of the appendix by proliferation of neural tissue.[1] It represents a hyperplastic proliferation of unmyelinated nerves and Schwann cells, possibly due to an increased number of extra-epithelial enteroendocrine cells.[2]
Case Report and discussion
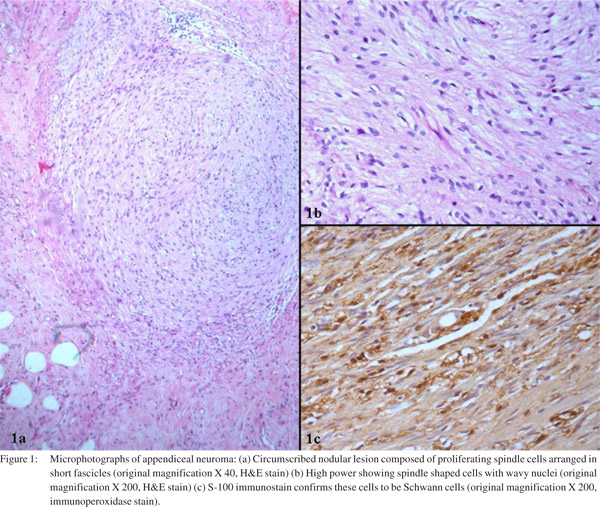
We report an incidental finding of an appendiceal neuroma in a 40-year-old male where intestinal resection was done following traumatic intestinal perforation. Grossly, the appendix measured 5 cm in length. The wall of appendix was thickened throughout its length with complete fibrous obliteration of the distal tip of the appendix. Microscopic examination of the section from the tip revealed a circumscribed nodular lesion (Figure 1a) completely disrupting the mucosa and obliterating the lumen. The lesion was composed of proliferating spindle cells arranged in short fascicles with elongated, wavy nuclei (Figure 1b). These cells were confirmed to be Schwann cells by S-100immunoreactivity (Figure 1c). In addition, there was an increased number of Schwann cells along with fibroblasts in submucosa admixed with few lymphomononuclear cells suggesting repeated attacks of inflammation which might be asymptomatic.
Neurogenous hyperplasia is a histopathological entity that can be identified by hematoxylin-eosin staining. History and clinical examination cannot differentiate preoperatively between acute appendicitis and neurogenic appendicopathy.[3] There is continuum of the disease process from appendices with intact lumens, featuring intramucosal neurogenous hyperplasia to obliterated specimens whose axial portions are composed of varying proportions of nerve tangles and fibrous tissue. Predominantly fibrotic specimens are considered as end-stage of this process. Repeated minimal subclinical attacks of inflammation are thought to trigger this lesion.[4] On lightmicroscopy, appendiceal neuromas appear as a loose proliferation of spindle cells usually in a myxoid background, frequently with entrapped fat and connective tissue and infiltrated by eosinophils. Majorities are located centrally in the appendix without nodule formation but occasional cases present with central nodularity. The spindle cells are positive for S-100 protein and neuron-specific enolase in all cases.[5]
Most cases of so called fibrous obliteration actually represent appendiceal neuroma. The pathogenesis of the process remains unknown. Some authors believe that these may be secondary to hyperplasia of neuroendocrine cells.[5] Neuromas usually show endocrine cells within the hypertrophied nerve bundles which may be the cells of origin for carcinoid tumor. As neurogenic appendicopathy can be diagnosed only histologically, it is to be encouraged that all appendicectomy specimens, even when macroscopically unremarkable should be examined.
References
- Masson P. Carcinoids (argentaffin-cell tumours) and nervehyperplasia of the appendicular mucosa. Am J Pathol. 1928;4:181– 211.
- Aubock L, Ratzenhofer M. “Extraepithelial enterochrmaffin cell—nerve fibre complexes” in the normal appendix, and in neurogenic appendicopathy. J Pathol. 1982;136:217–26.
- Franke C, Gerharz CD, Bohner H, Ohmann C, Heydrich G, Krämling HJ, et al. Neurogenic appendicopathy in children. Eur J Pediatr Surg. 2002;12:28–31.
- Olsen BS, Holck S. Neurogenous hyperplasia leading to appendiceal obliteration: an immunohistochemical study of 237 cases. Histopathology. 1987;11:843–9.
- Stanley MW, Cherwitz D, Hagen K, Snover DC. Neuromas of the appendix. A light-microscopic, immunohistochemical and electron microscopic study of 20 cases. Am J Surg Pathol.1986;10:801–15.
|